by Liz Hillman EyeWorld Senior Staff Writer
Experts discuss the challenges of dysfunctional lens syndrome, amblyopia, ocular surface disease, and vision restoration
Over the last 3 decades, modern refractive surgery has grown to seven procedures (eight if you include refractive cataract surgery). The stalwarts of corneal refractive surgery—PRK and LASIK—have been refined in patient selection, risk mitigation, technology, and complication management to the point where patient satisfaction with vision after LASIK in the PROWL studies ranged from 96–99%, and patient satisfaction with surgery ranged from 98–99%.1
Relative newcomers—small incision lenticule extraction (SMILE), intracorneal inlays, phakic IOLs, refractive lens exchange, and crosslinking—have expanded refractive options beyond corneal-based procedures, made inroads into presbyopia correction, and are starting to find their place within the market. With so many options available, just selecting the right procedure for the patient is considered a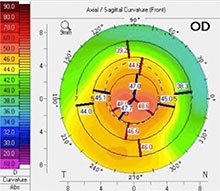
challenge by today’s refractive surgeons. The ophthalmologists EyeWorld spoke with about challenges in refractive surgery each cited the paradigm shift that has come about with the options available to patients seeking better vision.
“The biggest challenge is figuring out which option matches the patient who is at a certain stage of life, at a certain stage of activities, hobbies, and work, and which one of these is going to suit the patient in terms of visual lifestyle but also be the best in terms of long-term stability and be the least risky,” said Neel Desai, MD, The Eye Institute of West Florida, Largo, Florida.
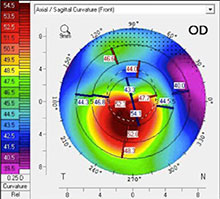
Crosslinking can halt the progression of keratoconus, but Dr. Donnenfeld describes how crosslinking can be combined with excimer laser treatment to then regularize the cornea. Source: Eric Donnenfeld, MD
In addition to this challenge, Dr. Desai, Daniel Durrie, MD, clinical professor and director of refractive surgery, University of Kansas Medical Center, Overland Park, Kansas, and Eric Donnenfeld, MD, Ophthalmic Consultants of Long Island, Garden City, New York, and EyeWorld chief medical editor, shared specific examples of what they consider challenging refractive surgery cases. A range of overarching themes were addressed, including the importance of patient education, ocular surface disease, and visual rehabilitation.
The middle-age patient requesting LASIK
A patient 48–60 years old comes in seeking LASIK, but a corneal-based procedure might not be the best option, Dr. Durrie said. While LASIK, PRK, or SMILE might all be possible for these patients, Dr. Durrie said, this age group has an underlying problem beginning in their crystalline lens that they probably don’t understand, and it might cause them to be unhappy with laser vision correction.
“The important thing right up front is to spend the time to educate them on what’s going on in their eye,” Dr. Durrie said, explaining that he will describe to patients the three stages of dysfunctional lens syndrome, what it’s doing to their lens, and how that will impact their vision now and in the future. After helping patients understand the changes that are causing them to develop presbyopia and eventually a cataract, then you can discuss refractive options with them.
Dr. Durrie said candidacy for laser vision correction can be discussed in the context that the patient’s lens will change and impact the visual outcomes of this procedure. The other option, he tells these patients, is refractive lens exchange, which can not only correct their refractive error but prevent cataract formation in the future as well.
Dr. Durrie said some patients still want a corneal-based procedure, even after the discussion of lens-based. He said the education about the changes in their lens “helps them not blame their future lens changes on the surgery you did.” Dr. Durrie has this same educational conversation with patients in their 20s and 30s, just so they’re aware of the changes that will happen decades down the road. It doesn’t keep them from choosing to have surgery, he said.
The amblyopic patient who wants refractive surgery
Another challenging case is the patient with amblyopia who comes in seeking refractive surgery. Dr. Durrie said he sees about one of these patients a week. “People who have had poor vision throughout their life are more likely to come in, so we see patients with amblyopia at a higher percentage than the general ophthalmologist or optometrist would,” he said.
Patients who are 20/15 or better in their dominant eye and have mild amblyopia of 20/25 or 20/30 best corrected in their nondominant eye can benefit tremendously from surgery, Dr. Durrie said. With these patients, he explains what a lazy eye is—how their brain learned to favor the good eye—and that refractive surgery will not fix that aspect of their vision. It’s expectation setting, he said. “You’re telling them they can have a surgery, but we can’t change the brain,” he said, adding that he’ll see these patients twice before surgery to make sure their prescription is stable. Another category is the patients whose amblyopia was missed or untreated in childhood and they are 20/200–20/400 best corrected. “They’ve been hoping all their life that someone could fix their lazy eye. This is a more important educational process because they’re not going to get a lot of benefit out of surgery,” Dr. Durrie said. While their myopia, hyperopia, and astigmatism can be corrected, they’re still likely to be no better after surgery. “It’s a real disappointment to them … but it’s important to help them understand that they’ve gotten along well and functioning to this stage; it’s something they’ve adapted to,” Dr. Durrie said. If they really want refractive surgery in their good, dominant eye, Dr. Durrie said this presents a dilemma because they only have one eye for functional vision. He proceeds with extreme caution in these cases and might even perform surgery on the amblyopic eye as a trial run, discounted or free of charge, before proceeding with the other eye. Finally, there are patients with strabismus with a lazy eye. Dr. Durrie said these patients’ strabismus can often get better with refractive surgery due to better vision getting them to hold their eye in a more regular position, but he’ll have them consult with an adult strabismus specialist before surgery because some patients can have an increase in their deviation.
The patient with disguised ocular surface disease
When a woman in her 40s came to Dr. Desai’s office seeking LASIK, she didn’t complain of dry eye symptoms. Careful examination, however, revealed not only dry eye but more serious ocular surface disease. This patient was a moderate myope but only corrected to 20/30 with glasses, which Dr. Desai said was a red flag when she wasn’t correctable to 20/20. With some manipulation, he was able to refract her to 20/20 but it fluctuated. Her cycloplegic refraction didn’t match her manifest refraction in terms of magnitude and axis of astigmatism. Preoperative topography revealed 3.5–5 D of corneal astigmatism. With these indicators, Dr. Desai examined her further, finding chronic underlying keratitis, dry eye, and a little bit of epithelial basement membrane dystrophy. Dr. Desai told the patient that he thought LASIK, at this time, was a bad idea due to her ocular surface disease and inconsistency of her preoperative measurements. “I told her that I’d rather do this the right way, regardless of what option we might choose, rather than do it the fast way,” he said. Establishing this trust with the patient, Dr. Desai moved forward with a superficial keratectomy with a PROKERA (Bio-Tissue, Doral, Florida) graft placed for 3 days. By the time the graft was removed, 100% reepithelialization was achieved. In the month following, Dr. Desai put the patient on a tapering dose of steroids and lifitegrast (Xiidra, Shire, Lexington, Massachusetts). After that month, the patient told him for the first time she could feel that her eyes were dry. This, Dr. Desai said, was actually a good sign because it indicated corneal nerve regeneration. The ocular surface disease was being treated and she was on her way toward candidacy for some possible refractive procedure. A month later her ocular surface was pristine with no keratitis and her topography revealed no astigmatism. “It occurred to me that if someone had done LASIK, her dry eye and ocular surface disease state would have been far worse off, and I may have been treating off a refraction that was so erroneous she would have been way off target,” Dr. Desai said. Discussing all of the different refractive options that were available to her, the patient opted for clear lens extraction with Tecnis Symfony extended depth of focus IOLs (Johnson & Johnson Vision, Santa Ana, California). Postop she was 20/20, J2+, and “wildly happy,” he said. From a technological standpoint, Dr. Desai said this case shows that you don’t necessarily need some of the more advanced biometric devices to diagnose a patient with ocular surface disease or corneal irregularities. You need vital staining, a detailed slit lamp exam, a retinoscope, and a phoropter, he said. “It doesn’t take huge capital expenditures … to identify some of these problems ahead of time,” Dr. Desai said. “What it does take is not technology but an interest in finding those things, a willingness to look for them and a willingness to treat them.”
The patient who can’t see well with glasses or contact lenses and could need a corneal transplant
Dr. Donnenfeld said to him, today’s challenging refractive surgery cases are the ones in which he is rehabilitating a person’s vision. “Someone who is having visual disturbances that are affecting their quality of life that can’t be fixed with glasses or even contact lenses, and what I’m offering patients is an opportunity to improve their vision and eliminate the need for corneal transplantation,” Dr. Donnenfeld said. Many of these cases are only now possible due to recent advances in technology. One example is the ability to rehabilitate the vision of a young person with keratoconus. Dr. Donnenfeld said he first evaluates if the cornea is stable; if not, he will perform corneal crosslinking. Once progression of the disease is prevented with crosslinking, the patient could be a candidate for topographic or wavefront-guided laser refractive surgery. “None of these treatments were in the United States a couple of years ago,” Dr. Donnenfeld said, noting FDA approval of crosslinking in 2016 and approval of the first topographic laser in 2013 and wavefront lasers starting in 2003. “Now I can take these irregular corneas, smooth them out, improve quality of vision, and many times take these patients out of gas permeable contact lenses and put them in soft contact lenses, very commonly glasses, or sometimes they can see without glasses completely. “This takes refractive surgery to the next generation. Before we were doing refractive surgery to remove the need for glasses, but now we can do refractive surgery to remove the need for corneal transplantation or gas permeable contact lenses,” he said. Another example is patients who have irregular corneas from scars, which might be due to trauma or viral infection. In some cases, these scars can be removed with a laser through phototherapeutic keratectomy (PTK)2 or a lamellar flap, created with a femtosecond laser. From there, the refractive error could be treated. There are also cases of corneal dystrophies, Dr. Donnenfeld said, that can be treated with PTK3 or lamellar keratectomies. “Not only are we doing rehabilitation with excimer lasers, we’re doing rehabilitation with femtosecond lasers as well,” Dr. Donnenfeld said. On the horizon is the ability to do stromal ablations to remove stromal scars using the SMILE technique; registration systems to more accurately map the cornea and treat irregularities; lamellar inlays with human corneal tissue that won’t be rejected; use of corneal inlays, such as KAMRA (CorneaGen, Seattle), to treat higher order aberrations in irregular corneas; and using lasers to treat irregular corneas prior to cataract surgery or, conversely, IOLs to improve the contour of the lenses to suit an irregular cornea to improve refractive outcomes, Dr. Donnenfeld said. “The goal of refractive surgery is to be able to rehabilitate patients with normal corneas and abnormal corneas as well,” Dr. Donnenfeld said. “There are many new technologies on the horizon.”
References 1.
Eydelman M, et al. Symptoms and satisfaction of patients in the Patient-Reported Outcomes With Laser In Situ Keratomileusis (PROWL) studies. JAMA Ophthalmol. 2017;135:13–22. 2. Alevi D, et al. Photorefractive keratectomy with mitomycin-C for the combined treatment of myopia and subepithelial infiltrates after epidemic keratoconjunctivitis. J Cataract Refract Surg. 2012;38:1028–33. 3. Miller A, et al. Prevention of recurrent Reis-Bucklers dystrophy following excimer laser phototherapeutic keratectomy with topical mitomycin C. Cornea. 2004;23:732–5.
Editors’ note: Dr. Desai has financial interests with Johnson & Johnson Vision, Alcon (Fort Worth, Texas), Novartis (Basel, Switzerland), and Bio-Tissue. Dr. Donnenfeld has financial interests with Johnson & Johnson Vision, Alcon, Bausch + Lomb (Bridgewater, New Jersey), TLC Laser Eye Centers (Mississauga, Canada), and Carl Zeiss Meditec (Jena, Germany). Dr. Durrie has financial interests with Johnson & Johnson Vision and Alcon.
Contact information Desai: desaivision@hotmail.com
Donnenfeld: ericdonnenfeld@gmail.com
Durrie: ddurrie@durrievision.com
Source: https://www.eyeworld.org/