Device Focus Pupil dilating devices Pharmacological vs. mechanical
by Rich Daly EyeWorld Contributing Writer
Amid the proliferation of pupil dilating devices, it remains important to know when cataract patients are best served by them or pharmacological options. If the patient’s pupil dilated well in the preop visit but does not seem as dilated on the operating table, Bonnie Henderson, MD, augments the topical dilation drops with intracameral epinephrine. “The preservative-free epinephrine can be drawn directly from the vial and diluted 1:4 with balanced salt solution and injected into the anterior chamber,” Dr. Henderson said. “I only inject a small amount—about 0.3 cc—turn off the microscope, and allow it to work for 1 minute before continuing the case.” The injection of epinephrine follows injection of preservative-free lidocaine into the anterior chamber. “I have found that epinephrine alone works well and does not seem to cause any discomfort to the patient,” Dr. Henderson said.
If the pupil does not dilate well in the clinic, Dr. Henderson will plan to use a device. “However, if the pupil dilated sufficiently but the patient is on a medication that can cause floppy iris syndrome, I will have the device ready in the operating room,” Dr. Henderson said.
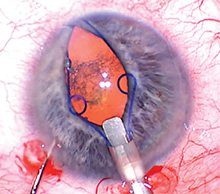
Richard Tipperman, MD, tries adjuvant pharmacological substances for small pupil cases and uses them prophylactically in all femtosecond cases. Additionally, surgeons at Wills Eye Institute use epi-Shugarcaine solution (epinephrine and lidocaine in fortified balanced salt solution) to enlarge pupils during cataract surgery. Mechanical devices Dr. Henderson turns to a mechanical device to help with pupil dilation and maintenance in other circumstances. In the preop evaluation in the clinic, Dr. Henderson evaluates the level of pupillary dilation. She also notes any medications the patient is taking that might affect the pupil. If the pupil does not dilate well in the clinic, Dr. Henderson will plan to use a device. “However, if the pupil dilated sufficiently but the patient is on a medication that can cause floppy iris syndrome, I will have the device ready in the operating room,” Dr. Henderson said. If the iris seems floppy at the beginning of surgery—even after the injection of intracameral lidocaine or viscoelastic—she implants a pupillary dilation device before creating the capsulorhexis. “If the capsulorhexis is already made and the pupil starts to constrict, it is still possible to use hooks or a ring at that time,” Dr. Henderson said. “However, great care must be taken to avoid capturing the edge of the capsule while attempting to capture just the edge of the pupil.” Dr. Tipperman said a poorly dilating pupil clearly is the leading indication in such situations but noted that there are additional considerations as well. “I’m more likely to use a mechanical device with a ‘small pupil plus,’ which is a small pupil plus a very dense lens, a small pupil plus pseudoexfoliation, or a small pupil plus a very shallow anterior chamber,” Dr. Tipperman said. Device selection When the pupil alone is the problem, Dr. Henderson prefers a ring type of device. “However, if I suspect that the zonules are also weak, then I prefer hooks so that I can use the hooks to keep the pupil dilated and to support the capsular bag. I like the adaptability of hooks,” Dr. Henderson said. “Also, with hooks, I can choose the location of the placement and can choose how many to use.” Another situation in which Dr. Henderson prefers to use hooks over rings is during scleral fixation of an IOL. “It is sometimes helpful to use a hook to give additional exposure to the area where the haptic is to be fixated,” Dr. Henderson said. Among situations or patient types where Dr. Henderson modifies her use of a device to dilate the pupil is during manual small or large incision cataract surgery when the lens must be prolapsed out of the capsular bag and into the anterior chamber. “This is very difficult to do with any type of pupillary dilation device in place,” Dr. Henderson said. “Therefore, in these cases, I recommend using a dilation device (either hooks or rings) to dilate the pupil in order to perform the capsule opening and remove the device before prolapsing the nucleus.” Another situation where a surgeon should take caution with pupillary dilation is in cases of patients with uveitis. “In some patients, the iris can become damaged or remain dilated if the iris is stretched with a dilation device,” Dr. Henderson said. “The device may be necessary to perform the surgery safely so it is still prudent to use one, but the surgeon should be aware that the pupil may not constrict back to the same preoperative size.” Dr. Tipperman also has tried multiple devices, but he prefers the Malyugin ring for dilation due to its ease of insertion, placement, and removal. However, Dr. Tipperman avoids the use of the ring in very small pupils or fibrotic pupils, where it can still produce sphincter tears. “Especially if I’m using a multifocal IOL in these cases, I try to avoid mechanical pupillary dilation,” Dr. Tipperman said.
About the doctors Bonnie Henderson, MD Clinical professor Tufts University School of Medicine Boston Richard Tipperman, MD Attending surgeon Wills Eye Hospital Philadelphia Financial interests Henderson
Contact information
Henderson: bahenderson@eyeboston.com
Tipperman: rtipperman@mindspring.com
Source: https://www.eyeworld.org/